Often times as interior designers we are responsible for specifying finishes and materials that contribute to a well-designed and coordinated interior environment. We spend valuable time researching and selecting the appropriate products to recommend to the client and our presentation work should always be a reflection of that.
The way we represent our work needs to reflect confidence in our ability to listen to the client, meet budget and performance expectations and bring a high level of creativity and coordination to the project.



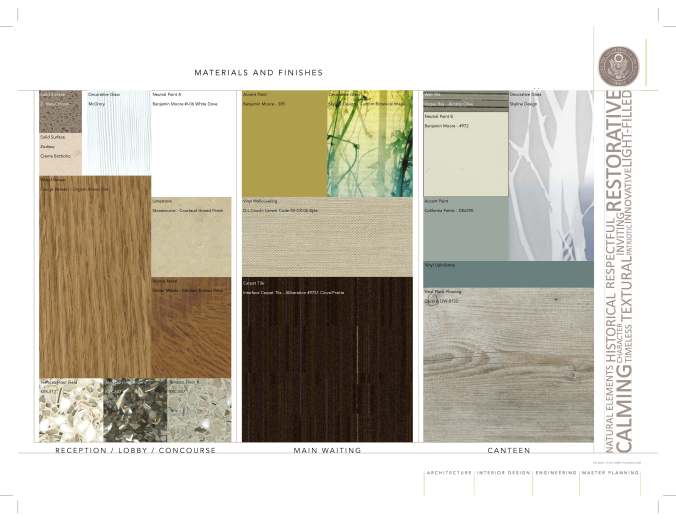
Here are some guidelines to follow that ensure a professional, organized and visually engaging materials board:
Basic Guidelines
- Identify the specific location where the products will be used and arrange accordingly
- Align materials to one another for an organized layout
- Arrange materials with flooring at the bottom, then wall finish and finally casework and interior glazing at top
- Size according to % used in an area
- Include major material components (its okay to omit rubber base, etc)
- Never show manufacturer labels or wording
- Never include paint or plastic laminate samples with pre-punched holes
Enhanced Elements
- Include key concept words to help visualize approach to the interior environment
- Include 3D concept sketches to highlight overall design of space support material selections
- Specific material information can be included, such as style name and #, color, manufacturer, etc. that coordinates with AI dwgs and specifications
- Where applicable include specialty decorative lighting or other elements that enhance space
When it comes to presenting materials to the client I much prefer to start with a curated set of loose finishes and material samples, sometimes adding color and pattern options. This allows the clients to touch and interact with the materials and feel part of the selection process. Actual sample boards where the materials have been cut and mounted to foam core don’t last long and tend to get picked apart. They end up sitting around looking beat up and old, and eventually get thrown away.
It is only after approval based on the loose samples that I create the materials presentation board digitally in InDesign and Illustrator or Photoshop. I use the digital boards for final client sign-off and a visual record that can be referenced by both the client as well as the design and construction teams. The digital materials are much easier to size and manipulate in a manner that visually represents their impact in the spaces they will be used. The digital boards can be printed and mounted for presentations and stored on the computer for future reference.




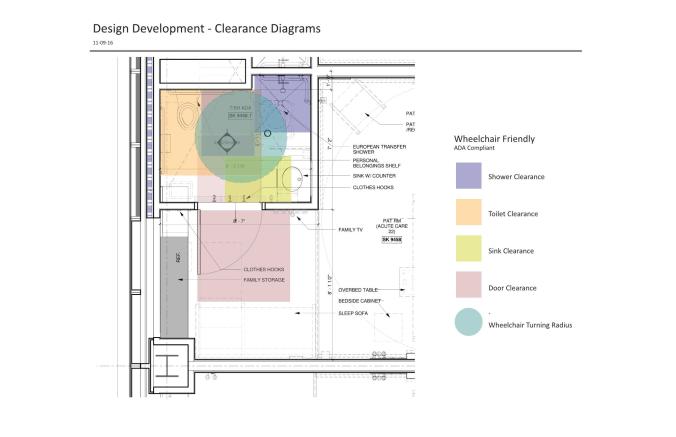 Fresh from planning new inpatient units through to design development my recent experience of designing code compliant patient toilets for 150 newly constructed rooms has given me insight on a few key planning considerations in the future will save me time and re-work (and possibly some sanity).
Fresh from planning new inpatient units through to design development my recent experience of designing code compliant patient toilets for 150 newly constructed rooms has given me insight on a few key planning considerations in the future will save me time and re-work (and possibly some sanity).







